
Science
 OUR FAVORITE NEUROTRANSMITTERS
OUR FAVORITE NEUROTRANSMITTERS
THE FOLLOWING represents a distillation of many article segments - past and present - spread across mcmanweb ...
The brain is a three-pound mass containing some 100 billion nerve cells - neurons - thousands of different kinds, each forming more than a thousand synaptic connections with other neurons. This is where neurotransmitters come in, chemical messengers that link neurons.
Neurotransmitters - An Overview
Forget about "chemical imbalance." Instead of conceptualizing the brain as some sort of uniform chemical soup that could use a bit more serotonin or dopamine, we need to see the brain as a highly intricate ecosystem, organized into micro and macro systems interconnected and interdependent.
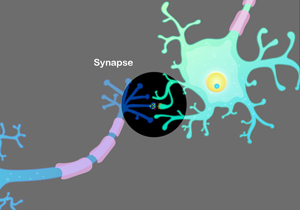
Neurotransmitters are synthesized inside the neuron. When things go right, signals from the neuron travel out a thread-like extension called the axon, which may end in several terminals. Just over the gap - synapse - are the target neurons with many protruding spines - dendrites - waiting for the mail.
You will hear talk of "presynaptic" and "post-synaptic" neurons, which are unavoidable fictions for teaching purposes. We pick up on the action in the "presynaptic" neuron, whose axon is primed for launching neurotransmitters.
All told, there are some 100 types of neurotransmitters in the brain. On release from the axon, certain neurotransmitters leap across the synapse and momentarily bind to specialized receptors along the dendrites of the "post-synaptic" neurons. The mail has been delivered.
From there, a complex series of signaling cascades follow that switch on or off or maintain no end of functions inside the target neuron.
Fast synapses are roughly divided into excitatory and inhibitory, with glutamate as the main excitatory neurotransmitter and GABA as the main inhibitory neurotransmitter.




The neurotransmitters we are most familiar with - dopamine, serotonin, and norepinephrine - involve slow and more complex transmission. They interact with signaling proteins found inside the cell membrane in a way which allows the receiving neurons to process signals from glutamate and GABA. According to the Surgeon General's 1999 Report on Mental Health:
To use a metaphor of a musical instrument, if glutamate, the excitatory neurotransmitter, is puffing wind into a flute or clarinet, it is the modulatory neurotransmitters such as dopamine or serotonin that might be seen as playing the keys.
Thanks to the neurons' axons and their ability to extend throughout the brain, their communicating neurotransmitters have the capacity to light up the entire nervous system. In the words of the Surgeon General:
These neurotransmitters are responsible for brain states such as degree of arousal, ability to pay attention, and for putting emotional color or significance on top of cold cognitive information ... It is no wonder that these modulatory neurotransmitters and their receptors are critical targets of medications used to treat mental disorders - for example, the antidepressant and antipsychotic drugs - and also are the targets of drugs of abuse.
The crowning complexity of the brain, according to the Surgeon General, is that it is not static. Every time a person learns something new, that experience alters the structure of the brain. Thus:
Experience that is salient enough to cause memory creates new synaptic connections, prunes away old ones, and strengthens or weakens existing ones ...
Glutamate and GABA
Glutamate (excitatory) and GABA (inhibitory) represent the yin-yang of the neurotransmitters, with both present in nearly all synaptic function all over the brain. The mood stabilizers used to treat bipolar are thought to act on one or the other or both.
SIGN UP FOR MY FREE EMAIL NEWSLETTER
There are two types of glutamate receptors, ionotropic (iGluR), including NMDA, kainate, and AMPA receptors; and metabotropic (mGluR), which mediate numerous chemical actions. When the NMDA receptor is working right, glutamate and glycine bind to the receptor, which opens up its corresponding ion channel and permits calcium entry into the neuron. This in turn promotes intracellular signaling essential to plasticity and survival.
Husseini Manji MD, formerly of the NIMH and now at J&J, reports on what can go wrong: In response to stress and mood episodes, glutamate reuptake in the synapse is compromised, resulting in increased calcium influx through the NMDA receptors and ion channels into the neuron and the activation of certain calcium-dependent enzymes that can result in cell atrophy and death. In some patients, Dr Manji observed, their mood disorder may be fundamentally atrophic (ie from brain cells in physical distress) rather than symptomatic.
GABA is formed in the brain from glutamate, glucose, and glutamine, and binds to one of two receptors on the postsynaptic neuron. GABA A receptors regulate excitability and anxiety, panic, and stress, and are the targets of benzodiazepines such as Ativan, as well as alcohol. In both cases, over time, the neuron structurally changes to accommodate increased GABA supply, setting up the potential for dependence and abuse. Other drugs of over-use and abuse work indirectly on GABA receptors.
Gerard Sanacora MD, PhD of Yale has used magnetic resonance spectroscopy to measure GABA in the brain, finding that those with melancholic depression show low GABA concentrations in the occipital cortex, while the depletion is not as pronounced for those with atypical depression, indicating a diagnostic potential for subtypes of depression.
As well, GABA and glutamate are also implicated in schizophrenia. John Krystal MD of Yale refers to "noise amplifying abnormality," resulting in chaos in the prefrontal cortex.
Dopamine
Dopamine has been implicated in depression and mania, not to mention schizophrenia, ADHD, addictions, and so on, plus assorted behaviors such as novelty-seeking and experiencing pleasure.
The neurotransmitter is manufactured by L-DOPA, which in turn is produced from tyrosine, or - more precisely - L-DOPA is converted to dopamine by action of DOPA decarboxylase (DDC). L-DOPA itself is converted from tyrosine by the action of tyrosine hydroxylase (TH).
"Phasic" dopamine release is characterized by burst firing and is thought to occur in response to behavioral stimuli, such as those that may predict reward. In contrast, "tonic" dopamine release is slow and irregular. The neurotransmitter is implicated in depression, bipolar, schizophrenia, psychosis, Parkinson's, ADHD, substance use, and aggressive behavior.
Most dopamine-producing neurons are located in areas near the brainstem. Their axons extend in one of three specific but overlapping paths (via the medial forebrain bundle) to stimulate specific cortical and subcortical structures. In contrast, serotonin and norepinephrine patterns of distribution are far more diffuse.


The nigrostriatal pathway (in the subcortical areas of the brain) has a prominent role in motor planning and movement, plus cognition.
The mesocortical pathway, which projects to the frontal and temporal cortices, is believed to be vital to concentration and executive functions such as working memory. The mesolimbic pathway, which projects into the limbic system, including the hippocampus and amygdala, is particularly important for motivation, the experience of pleasure, and reward.
Cocaine and various forms of meth are notorious for enhancing dopamine production (ADD meds and Parkinsons meds do so in a less dramatic way), while antipsychotics bind to dopamine D2 receptors and thus inhibit too much of a good thing. Unfortunately, antipsychotics don't just limit themselves to the D2 receptors in the mesolimbic pathway, leading to what Stephen Stahl of UCSD calls a "high cost of doing business."
With street drugs, neurons structurally change over a short time to accommodate the increased dopamine supply, setting the scene for dependence and abuse. Other drugs of over-use and abuse may work primarily on other neurotransmitter systems, but all have the downstream effect of increasing the production of dopamine in the pleasure and reward circuits.
In depression, lack of dopamine, among other things, would account for lack of pleasure. In mania, too much dopamine is viewed as rocket fuel.
Serotonin
Serotonin (5HT) is best known for its antidepressant effect. The neurotransmitter is synthesized in the neuron from the amino acid tryptophan, which is converted to 5HTP, then to serotonin. It is released into the synapse in a similar fashion to norepinephrine. Serotonin has some 17 different types and subtypes of receptors, which underscores its importance as a neurotransmitter. Serotonin-producing neurons project from the raphe nucleus in the brainstem to the basal ganglia, frontal cortex, hypothalamus and limbic system, and down the spinal cord. Serotonin is also found in the GI tract, thus implicating itself in a host of functions, from mood to anxiety to sleep (serotonin makes melatonin, which regulates sleep) to sexual response to food craving and (in)digestion.
A presynaptic transporter sucks up excess serotonin from the synapse in preparation for the next release of the neurotransmitter. SSRI antidepressants are believed to work by binding to this reuptake pump, thus keeping more serotonin in circulation. Were this completely true, however, antidepressants would have an immediate effect, instead of taking at least two weeks to start making an impression and another two to six weeks to achieve full clinical benefit.
One explanation is that blocking the transporters desensitizes the neuron in a way that dampens normal firing for four weeks. Another explanation is that antidepressants also work on intracellular processes downstream of the neurotransmitters.
Serotonin drugs of abuse include ecstasy and LSD.
In depression, lack of serotonin would explain over-obsessing on grieving thoughts. Not surpsingly, serotonin meds also help with OCD.
Norepinephrine
Norepinephrine (also referred to as noradrenaline) is manufactured in the neuron by enzymes acting on the amino acid tyrosine, which convert it into L-DOPA, then to dopamine. Some of the dopamine is then converted to norepinephrine. Just as norepinephrine is created by enzymes, it can also be destroyed by enzymes, such as MAO (which also destroys serotonin and dopamine). Hence the MAO inhibitors that represent the first family of antidepressants.
Another first-generation class of antidepressants, tricyclics such as Elavil, have a dual reuptake action on both norepinephrine and serotonin. The later-generation SNRIs such as Effexor work in a similar fashion.
Most of the norepinephrine action takes place in an area of the brainstem known as the locus coeruleus, which monitors external stimuli and our responses (such as fight or flight) and pain. Norepinephrine and the locus coeruleus are also believed to play a role in cognition, mood, emotions, movement, and blood pressure. Difficulty concentrating, fatigue, apathy, and depression are some of the things that can result from norepinephrine going AWOL.
In depression, the prevailing theory is that lack of norepinephine is what accounts for psychomotor retardation. In anxiety, too much of the neurotransmitter is seen as part of the stress reaction.
Other Neurotransmitter Systems
Acetylcholine - Damage to this system has been linked to Alzheimer's. Cholinesterase inhibitors such as Aricept are believed to work by preventing the breakdown of acetylcholine. Specific nicotinic receptors in the acetylcholine system are linked to nicotine addiction, but safe alpha7 nicotinic agonists (for improving cognition) are being investigated for the treatment of schizophrenia.
Oxytocin and Vasopressin - As both neurotransmitters and hormones, these two peptides mediate a range of physical and mental functions, but their role in pair-bonding has earned them the reputation as the "love hormones."
Opioids - Endorphins are a popular term to describe complex chemical activity involved in killing pain, inducing sleep, and creating sensations of pleasure. Opiates such as heroin and morphine and opiate-derived pain-killers such as codeine and oxycodone appear to mimic natural endorphin activity by binding to opiate receptors. The immediate effect is blocking pain and causing drowsiness. A domino effect results from reduced GABA release failing to inhibit dopamine release. Medications such as methadone are aimed at mimicking the mimickers. Naltrexone, on the other hand, works by countering the opiate effect and blocking cravings.
Adenosine - Caffeine gets its effect by binding to these receptors, thus blocking fatigue-inducing adenosine neurotransmitters. A downstream effect is mild dopamine release. Once the blockade wears off, however, adenosine comes back into play, which is why coffee is only a temporary fix. The only cure for missing out on sleep is - drumroll - catching up on sleep.
Hypocretins - Also called orexins, these neuropeptides have recently been identified in sleep regulation. Breakdown in hypocretin function is believed to result in narcolepsy. The novel wakefulness agents Provigil and Nuvigil are believed to act on hypocretin.
Endocannabinoids - These compounds function as both neurotransmitters and hormones. Recent research reveals this system plays a major role in the body and brain in maintaining homestasis (stability). This involves processes as diverse as weight regulation and mood. Marijuana, which acts on this system, in small doses may act to promote homeostasis. In larger - recreational - doses - it may have the opposite effect.
Substance P - In the spring of 2003, this peptide, which is released in response to stress, was ready for prime-time, with Merck staging a coming-out party in the form of a well-attended dinner symposium (featuring two of the top academic psychiatrists Alan Schatzberg and John Rush) at that year's American Psychiatric Association's annual meeting. Phase II drug trials sponsored by Merck had already indicated its substance-P-blocker MK-0869 to be as effective as Paxil. Alas, the Phase III trials proved MK-0869 a dud, and in Aug 2003 Merck withdrew the drug from FDA consideration. Sayonara substance P.
Again, the Brain is Not Chemical Soup
Our near-exclusive focus on neurotransmitters tends to blind us to the complexity of the brain, such as what goes on inside the neuron, how brain systems interact, and the interplay between genes and environment. Don't stop reading now. Please check out: Inside the Neuron * Dopamine - Serotonin's Secret Weapon * Systems in Collapse * and Psychiatry's Big Bang.
See also: Our Favorite Hormones
This consolidates earlier articles, May 24, 2011, reviewed Dec 11, 2016
NEW!
Follow me on the road. Check out my New Heart, New Start blog.






