
Treatment
 THE CHEMICAL IMBALANCE MYTH
THE CHEMICAL IMBALANCE MYTH
The brain is not chemical soup that can use more serotonin.
by John McManamy
The brain is not chemical soup that can use more serotonin.
by John McManamy
SAYS HAMLET:
I have of late - but wherefore I know not - lost all my mirth, forgone all custom of exercises; and indeed it goes so heavily with my disposition that this goodly frame, the earth seems to me a sterile promontory …
Yes, we know depression when we see it, but what precisely are we talking about? Feeling sad? Lack of motivation? Psychic numbing? Is it a "normal" reaction to abnormal events or an abnormal reaction to normal events? A loss of energy or a mammalian need to hibernate? A crisis of the soul? Perhaps it's even a part of our normal personality. Hamlet did a lot of talking, but psychiatry can at best only hazard educated guesses at the true shade of his "nightly colour."
Obviously, no two depressions are alike, which makes one wonder why psychiatry treats them as if they are. When all is said and done, any medication is the right medication, so long as it is administered to the right person for the right condition. ButPharma - with psychiatry in compliance - promotes the myth of some kind of universal "chemical imbalance in the brain."
Thus in a Zoloft ad:
Note that the representation of the neuron is virtually empty. Here is a far more accurate micro-version of what is going on inside the neuron.
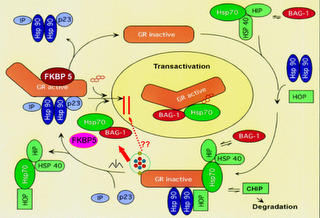
And here is a macro-version (with the red arrows representing back and forth neurotransmitter traffic involving countless neurons in certain sections of the brain):
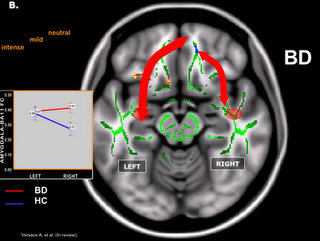
What this means is that instead of conceptualizing the brain as some sort of uniform chemical soup that could use a bit more serotonin or dopamine, we need to see the brain as a highly intricate ecosystem that requires sophisticated nurture and cultivation.




Think of the Brain as an Ecosystem, Instead
As you can guess, "macro" and "micro" are interconnected. Each regulates the other in highly intricate and virtually infinite ways. When things go right, we can only marvel at this creation of nature. When things go wrong, it's not just a chemical imbalance - it's a catastrophe, a collapse. Think "ecosystem."
If we were truly talking about chemical imbalance, the evidence would be revealed in the cerebrospinal fluid (CSF) of unmedicated patients. Serotonin that is not recycled in the brain is metabolized as 5-HIAA. Likewise, dopamine is broken down to HVA. The levels of these metabolites in the CSF are acknowledged to relate to the levels of their corresponding neurotransmitters in the brain. Over the course of fifteen years to the mid-seventies, researchers found that the various metabolite levels in patients were no different than those in the general population.
SIGN UP FOR MY FREE EMAIL NEWSLETTER
In other words, no chemical imbalance - or at least no uniform chemical imbalance throughout the brain. The picture that emerges from brain scans is compromised neurotransmitter signaling along specific pathways in the brain. The impact may be diffuse, but is hardly uniform.
Indeed, "imbalance" only makes sense in the context of neurotransmitter systems in opposition, as in "too much" or "too little" occurring in different parts of the brain at once. But our meds are too dumb to figure this out.
In his 2010 book, "Anatomy of an Epidemic," Robert Whitaker argues that rather than actually correcting chemical imbalances antidepressants in fact create them. With the administration of an SSRI antidepressant, we have learned over the years, the brain attempts to compensate by turning down serotonin release in presynaptic neurons and reducing the density of serotonin receptors in postsynaptic neurons. This is the brain's attempt to maintain homeostatsis (equilibrium), to keep serotonin at levels as they were prior to the introduction of the drug.
Only after two weeks or more does the antidepressant begin to assert itself. The brain's compensating mechanisms break down. Serotonin now floods the synapse and latches onto postsynaptic receptors. If you are the right individual with the right kind of depression, you are very lucky indeed. But can psychiatry tell in advance if you will be one of the lucky ones? The short answer is no, but a lot of inspired guessing is going on, namely:
Stress-Based Depression
In 2000, Ronald Duman of Yale discovered that new and old generation serotonin antidepressants (as well as exercise) promote new brain cell growth in the brain's hippocampus. The hippocampus, amongst other things, is involved with the temporal lobe in laying down new explicit memories and is in a dialogue with the amygdala regarding emotional memory. Hippocampal neurons are packed with glucocorticoid receptors, which make them vulnerable to stress.
This raises the obvious question: Do SSRIs work best for depression that is stress-based, either in repairing or replacing damaged hippocampal neurons or in protecting against stressful events? We don't know. Clinical trials do not test for this.


Over-Ruminating Depression
Helen Mayberg of Emory University has had promising results on depressed patients with deep brain stimulation (DBS), a surgery FDA-approved in the treatment of OCD. The patients Dr Mayberg is working with had not responded to antidepressants. DBS involves inserting an electric lead into the folds of the brain adjoining a particular area of the cingulate cortex. The anterior cingulate cortex (ACC), among other things, is involved in filtering out thoughts. Patients with OCD tend to lock into one thought. Many individuals with depression tend to over-ruminate. In both cases, the signaling from the lead is intended to break up this type of destructive thinking.
The ACC is tied into the serotonin system, which is why SSRI antidepressants work for OCD, but obviously not everyone with OCD (or depression). Although surgery is not about to become a universal treatment for depression, it stands to reason that what we learn from DBS may be applied to finding a better serotonin medication. At least we hope.
Vegetative Depression
Kitty Dukakis' book, "Shock," chronicles how ECT cleared up her debilitating depression after meds and other treatments failed. But it seems, perhaps, that she had already been successfully medicating her depression over the course of nearly a quarter century, only they were calling it drug abuse. Her depression set in only after she was treated for her addiction and weaned off her stimulants.
Or, perhaps the stimulants structurally changed her healthy brain to an unhealthy one, to the point where she was dependent on the uppers to keep her from being depressed.
Either way you look at Ms Dukasis' experience, we see a tie-in between certain types of depression and the brain's dopamine system. Dopamine, among other things, is involved in pleasure and reward and cognition. An overstimulated dopamine system can bring on erratic thoughts and behavior and psychosis. An undersupply of dopamine to certain areas of the brain can result in fatigue, loss of pleasure, and sluggish thinking. The success of serotonin antidepressants has caused us to overlook the potential of dopamine. Perhaps a safe and smart dopamine med could prove effective for certain kinds of "vegetative" depressions. Is anyone out there listening?
Antidepressant Take-Home Message
I just showed you three different types of depression, apparently centered in different areas of the brain, involving apparently different brain systems. I could have showed you a lot more. On the surface, all three depressions may appear the same, but beneath the hood something clearly different is going on with each one. It gets complicated, as nothing in the brain - on either a micro or macro level - operates in a vacuum. Neither can depression or any other mental condition be strictly localized to a particular area of the brain. But hopefully my point comes in loud and clear:
Depression is simply a term of convenience for several or dozens or hundreds of conditions in the brain that we do not understand. An antidepressant, then, is a misnomer, as it is simply the wrong pill for way too many depressions. An antidepressant may work against certain types of depressions, but we don't know which ones and on which individuals. And we will never know because the drug companies have no financial incentive to find out.
Thus, we become guinea pigs. "Try this and see if it works." Sorry, that's not good enough for me - or you, either, I can imagine. Fortunately, we don't have to wait for things to happen.
Next article: Antidepressants - Five Things You Need to Know
Previous Articles: Antidepressants - The Bad News First *Antidepressants - Right Med, Wrong Illness?
Reviewed June 30, 2016
NEW!
Follow me on the road. Check out my New Heart, New Start blog.






